Impactful by Design.
Through the commitment of thousands of generous participants, ARIC has helped to transform healthcare with breakthrough knowledge on the prevention and management of heart disease and related conditions.
ARIC is unique, both in its large size and over 30-year history, as well as how it bridges individual participant data with what is going on in their local communities. And like our participants, ARIC keeps going as we continue to ask new questions.
Many ARIC discoveries have increased our understanding of the causes of atherosclerosis and cardiovascular disease, advanced cardiovascular disease prevention, and shaped guidelines for treating coronary heart disease, diabetes, stroke, and chronic kidney disease.
We look forward to engaging future generations to better understand our health and do ever more "research with heart."

Goals
ARIC's goals are:
- To investigate the causes of atherosclerosis, a disease marked by plaque build-up in the arteries.
- To measure how cardiovascular risk factors, medical care, and outcomes vary by race, sex, place, and time.
- As ARIC's participants have gotten older, an additional goal has been to better understand the connections between cardiovascular health and cognitive function.
Project Scope
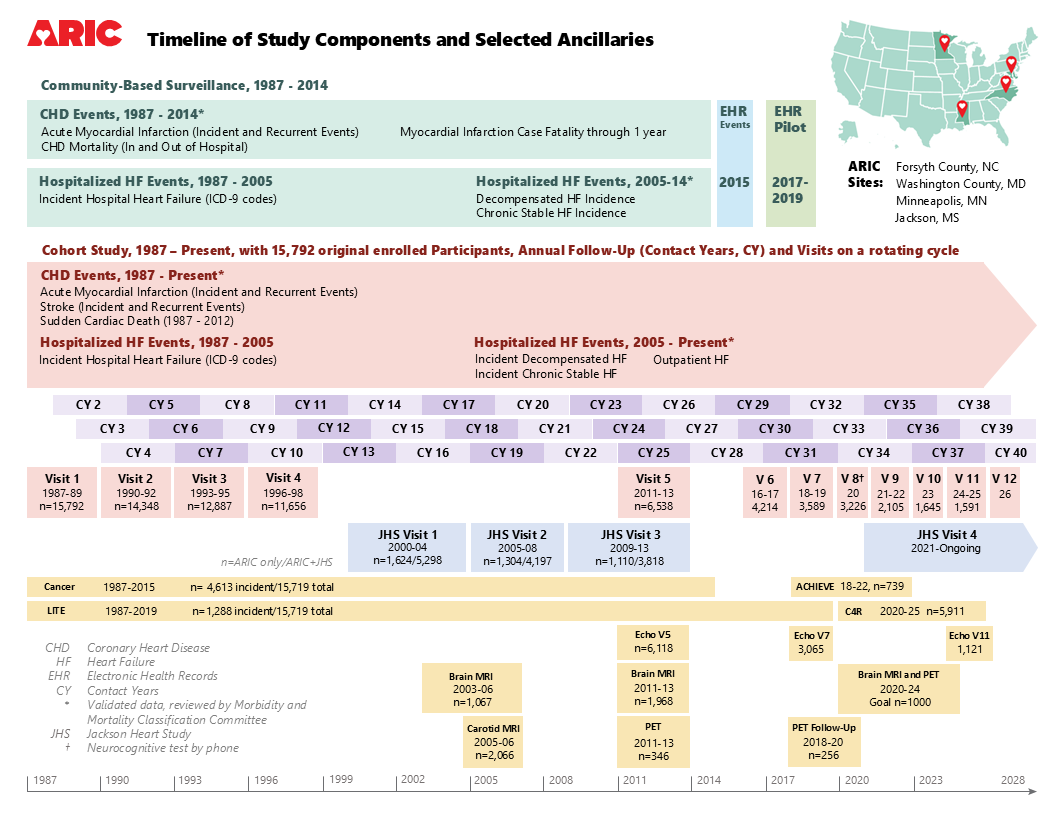
ARIC includes two key components: a cohort study and community surveillance. Ancillary studies are an important facet that span both components.
Cohort Study
The cohort study (1987 to present) recruited participants from four communities: Forsyth County, North Carolina; Jackson, Mississippi; eight northwestern suburbs of Minneapolis, Minnesota; and Washington County, Maryland.
The cohort study focuses on regular clinical exams, along with telephone follow-up twice a year to stay in touch with participants and assess health. Many of the participants who began the cohort study in 1987-89 are still active in the study today.
Findings from the cohort study have shaped clinical guidelines that doctors use to treat coronary heart disease, diabetes, stroke, and chronic kidney disease.
Community Surveillance
Community surveillance was conducted from 1987 to 2014 and focused on local data about hospitalizations and deaths due to coronary heart disease in the same four geographic areas as the cohort study, to better understand community trends and make comparisons to the cohort group.
This work has helped assess rates of heart attack, hospitalizations from heart failure, and deaths due to heart disease in over 400,000 adults.
Ancillary Studies
Over time, research questions have led to additional studies and investigations, some using the existing ARIC data and some contacting ARIC participants for new information.
Almost 300 ancillary studies have been funded to date and these studies are continuing to provide valuable information and answer important questions. Some recent examples include studying genetic markers associated with heart failure to help identify possible targets for new medicines, trying to understand why individuals with cancer appear to age faster, and the relationships between the microbes in our gut and problems with our memory and thinking as we age.
Funding Source
The Atherosclerosis Risk in Communities study has been funded in whole or in part with federal funds from the National Heart, Lung, and Blood Institute (NHLBI), National Institutes of Health (NIH), Department of Health and Human Services, under Contract numbers (75N92022D00001, 75N92022D00002, 75N92022D00003, 75N92022D00004, 75N92022D00005).
Additional funding has been provided by the NHLBI and other funding sources for a number of ancillary studies.
Timeline
ARIC has operated continuously since 1987 and is currently funded through 2028.
Please click here for a downloadable version.